
What is the proportion of women in medicine?
According to the World Health Organisation (WHO), women represent 67% of the global health and social care workforce. However, if we focus only on the field of medicine, this percentage decreases due to the need for higher education and the late evolution of the incorporation of women into the labour market, particularly in the most qualified professions.
In Spain, according to the National Statistics Institute (INE) survey on Registered Health Professionals, 53% of registered health professionals in 2023 were women. This figure exceeded that of men for the first time in 2017, and has increased year on year since then.
But the data also show that there is no parity in senior positions. Figures from the WOMEDS study - promoted by the Federation of Spanish Scientific Medical Associations (FACME) and published in 2023 in the journal BMC Human Resources for Health- show that, although 61% of the medical staff in Spanish public hospitals is made up of women, they only occupy 27.6% of service chiefs.
As stated in the update of the Report on the supply and need for specialist doctors in Spain (2023-2035) published by the Ministry of Health, ‘since medicine is a highly feminised profession (more than half of the doctors registered in Spain are women), a gender bias has been identified in healthcare leadership, in academia, research and institutional leadership in medical associations and scientific societies’.
Why don't women reach higher positions of responsibility?
For Carme Valls, a medical doctor specialising in endocrinology and medicine with a gender perspective and director of the ‘Women, Health and Quality of Life “ programme at the Centre for Analysis and Health Programmes (CAPS), the answer is clear: ”For the same reason that they don't become directors of almost anything in all other areas of society,’ she explains in conversation with SMC Spain. ‘There is a resistance on the part of men to give up power or share it,’ she stresses.
Valls points to motherhood as the second obstacle in the working life of female doctors: ‘It is seen as a burden that interrupts the professional career’.
One of the coordinators of the WOMEDS project, Pilar Garrido, head of the Medical Oncology Department at the Ramón y Cajal University Hospital and former president of FACME, explains more key factors: ‘There are many factors involved, including a lack of visibility, the impostor syndrome and the absence of female role models in leadership positions.
In addition, ‘we must also take into account gender inequality in the assignment of organisational or care tasks, which hinder professional development and reduce opportunities to achieve leadership positions,’ Garrido tells SMC Spain.
The oncologist comments that ‘the pandemic may have been a setback if international publications are anything to go by’. ‘The reason was that women and men spent the same hours working in the hospital, but outside, women spent more time caring for the family and home, while men spent more time on scientific production. This can have a differential impact on the curriculum, slowing down the professional development of qualified women in the short/medium term,’ says Garrido.
What is the importance of having women in these positions, as well as in medicine in general?
The former president of FACME is clear: ‘We cannot afford to lose half of the talent. ‘It is important to reflect the diversity of the world we live in in leadership positions,’ she stresses.
Valls points out that ‘if there are no women and no diversity in leadership centres and research groups, women are biased’. ‘They are not recognised and their differences are not studied,’ she says.
The inclusion of women in management positions has ‘a positive impact on healthcare, promoting a more inclusive and empathetic culture,’ Virginia Izura, deputy secretary of the General Council of Medical Associations (CGCOM) and coordinator of the Gender and Profession Observatory, tells SMC España.
Along the same lines, María Dolores Gallego, member of the Working Group on Women's Care of the Spanish Society of Primary Care Doctors (SEMERGEN), comments that ‘countries with a higher percentage of women in positions of power tend to adopt more rigorous policies’.
It is also important to bear in mind that gender balance has a direct impact on healthcare outcomes for patients and the general population. Indeed, a study published in the Annals of Internal Medicine indicated that patients treated by female physicians have lower rates of mortality and hospital readmission. In addition, ‘the benefit of receiving treatment from female physicians is greater for female patients than for male patients,’ the authors noted.
In which specialities do we find more or fewer women and why?
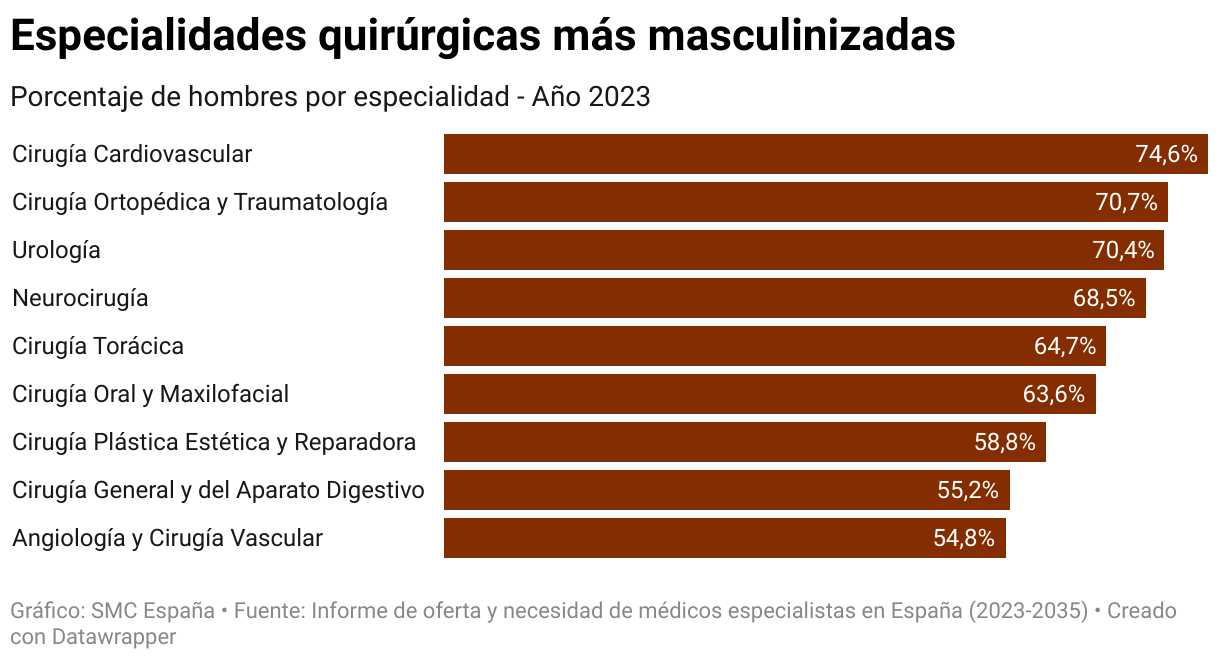
In general, surgical specialties -except for paediatrics- are the most male-dominated. Specifically, according to the Report on the supply and need for specialist doctors in Spain (2023-2035), the three specialities with the highest percentage of men are: cardiovascular surgery (74.6 %), orthopaedic surgery and traumatology (70.7 %) and neurosurgery (68.5 %).
On the other hand, in paediatrics in PC there are almost four women out of every five specialists, and in obstetrics and gynaecology, three out of every four specialists are women.
‘Of all the women who finish their degree, only 25-30% choose surgical specialties,’ says the deputy secretary of the CGCOM.
Valls explains the reasons: ‘Many opt for less demanding specialities, without so many hours of surgery, in which they can combine motherhood and care’.
In addition, the endocrinologist comments that the specialities are sometimes not adapted to women's bodies. ‘Surgery tables and equipment are not ergonomically adapted,’ she points out.
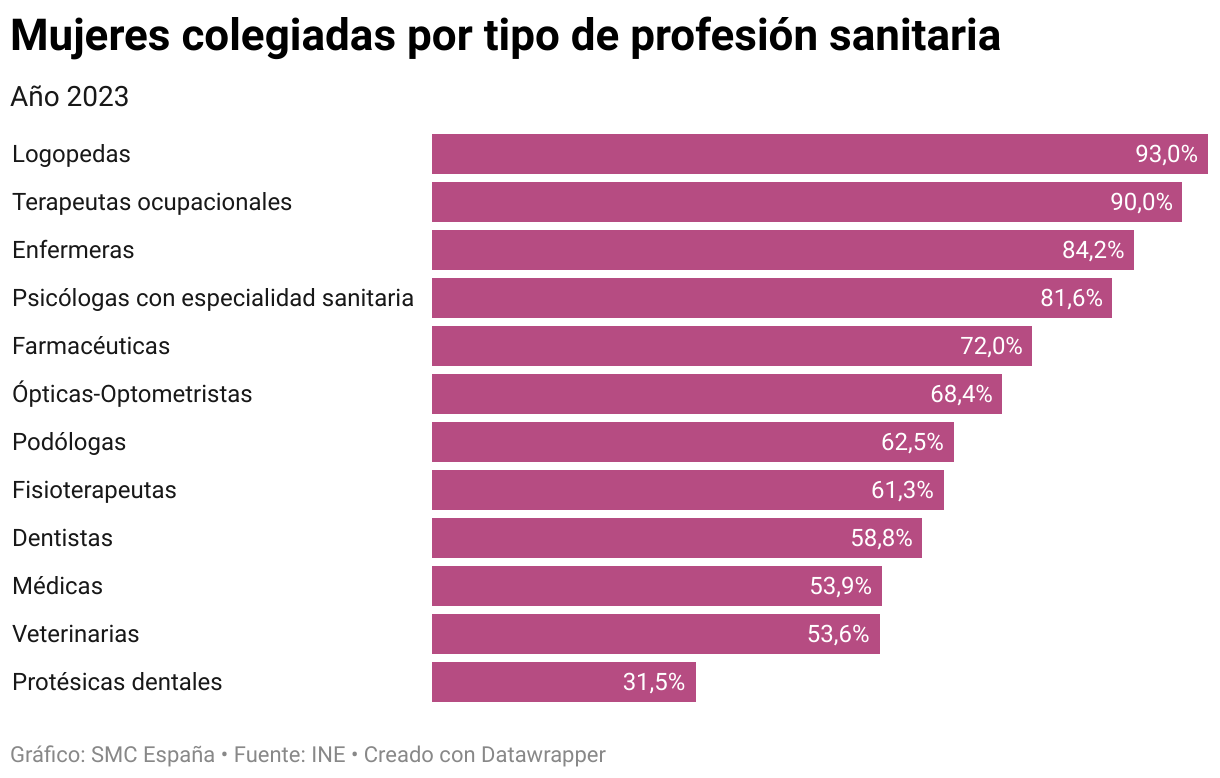
Meanwhile, INE data from the Registered Health Professionals Statistics show that in 2023 there were more women than men registered in 13 of the 15 professions analysed. The groups with the highest percentage of women were speech therapists (93 % were women), occupational therapists (90 %) and nurses (84.2 %).
In contrast, the types of profession with the lowest rates of femininity were dental technicians (31.5%), health physicists (32.2%) and veterinarians (53.6%).
What are the most common inequalities in the profession?
The main inequality, as Garrido points out, is ‘that there are not enough women doctors in leadership positions’. ‘They have to fight harder to be heads of research, work or services,’ agrees Valls.
This is not only the case in the heads of service in Spain's public hospitals, but also in the various Medical Associations and medical societies.
In the history of the presidency of the Spanish Medical Association ( 1921-present) there is not a single woman among the 21 people who have held the post. Of the 52 Medical Associations in Spain, only ten (19 %) - those of Ourense, Guipuzkoa, La Rioja, Ávila, Valencia, Toledo, Ciudad Real, Córdoba, Huelva and Granada - have a woman president.
Also, only ten of the 46 medical societies in the FACME had a female president during the first period of the WOMEDS study. In its second update, this figure rose to 12.
These data exemplify one of the conclusions drawn from an article published in the journal Social Science & Medicine: ‘Women doctors, although present, have been incorporated into a rigid environment, built without the intention of their flourishing’.
Moreover, as Gallego points out, ‘female doctors in senior positions have a slightly younger average age compared to men’. This ‘could be reflecting a double discrimination, by age and sex’, although she insists on the need for a more in-depth analysis of this situation.
There are also inequalities in terms of salaries. According to the WHO, in Spain there is a pay gap of around 15% against women in healthcare, after adjusting for different occupational categories. There are 17 countries with a smaller gap than Spain among the 26 analysed.
What are the most effective measures to tackle this inequality?
One of the aspects to consider, according to Garrido, is training aimed especially at women in the early stages of their professional careers, ‘aimed at providing tools to increase confidence in their abilities and to value their achievements, counteracting the famous impostor syndrome’.
As an article, published in the Journal of Medical Internet Research, points out, the aim is for this support to continue throughout women doctors' careers. ‘As women become true competitors for the limited resources in their fields, they are exposed to the pervasive culture of inequalities and systemic biases in academic medicine,’ the paper notes.
An article published in the Austrian journal Wiener Medizinische Wochenschrift states that future generations (Generation Y, Generation Z) are likely to accelerate changes towards a better work-life balance. ‘Gender balance can enhance the group process and improve the level of collective intelligence,’ the publication notes.
More specifically, Gallego comments to SMC Spain on the need for ‘decisive action with policies and funding to be applied in all areas, public and private, on gender perspective’.
Izura agrees: ‘It is crucial that effective policies continue to be implemented to ensure that women can access the same levels of responsibility and leadership as men, which will not only benefit women professionals, but also the health system as a whole.
What is gender-sensitive medicine and why is it important?
The gender perspective, in any field, is the study of the gender of the people who participate in a work, research or on whom the results of these are applied. ‘It means introducing it into the research work, differentiating it well and analysing these results at the end,’ explains Valls.
‘It seems unbelievable, but in medicine this is not done,’ says the endocrinologist. Valls comments that many diseases, including diabetes and cancer, take up to two and a half years longer to be diagnosed in women than in men. ‘There is a gender bias in the way we have taught medicine in the faculties. We have not taken into account the differences,’ she says.
‘Many other aspects that were not taken into account need to be introduced into the research work: the environment, working and living conditions and power relations. ‘We need to build a science of difference and inequality, to take both into account and teach them in the faculties,’ adds Valls.



