
It was Judah Folkman, a renowned American researcher, who said: “If you have cancer and you’re a mouse, then we’ll be able to take good care of you.” He said this in the 1990s, after discovering a compound capable of eliminating various tumours in laboratory mice with hardly any side effects, whilst many media outlets heralded it as a miracle cure and James Watson himself, the co-discoverer of the DNA double helix, claimed in the New York Times that Folkman was “going to cure cancer within two years”.
However, in clinical trials with patients, its effect was considerably less. Far from the miraculous promise, thirty years later, its use has not been approved in Europe or the United States.
It is often said in certain circles that we have cured cancer in mice thousands of times. However, when these results in animals are tested in the form of clinical trials in humans, they are successful only around 10% of the time — moreover, success here is not synonymous with a cure; it is usually an improvement in survival or quality of life. And the picture is not much different when many other diseases are taken into account. At the same time, the vast majority of Nobel Prizes in Physiology or Medicine involve research using laboratory animals, mainly mice, which have been employed to test virtually all available treatments.
The success rate may seem low, although “without them it would be 0%”, explains Lluís Montoliu to SMC Spain, a researcher at the National Centre for Biotechnology (CNB-CSIC), former chair of the CSIC Ethics Committee and a member of the Ethics Panel of the European Research Council (ERC).
Below, we explain why animals are used in research and why mice are the most commonly used, their advantages and limitations, the steps involved from the point a treatment appears effective in them until it can be determined whether they work in humans, the average timescales and success rates, the characteristics of certain disease models, and how results should be communicated to inform without raising false hopes—and whether it is sufficient to simply state “in mice”.
Why are animals needed in research, and what purpose do they serve? Why are mice the most commonly used?
Animal testing aimed at trialling and developing treatments provides information that, at present and in most cases, seems difficult to obtain by other means. “Much of this research cannot be carried out unless it is conducted within a complex system, within a living organism. Anyone who says it isn’t necessary simply doesn’t understand the situation properly,” argues Montoliu. Some of the data it helps to obtain relates to a drug’s efficacy, how it is absorbed and eliminated, where and how it acts, its possible side effects, or the most reasonable and appropriate starting dose. Without that information, the vast majority of therapies would not even have been able to begin human trials.
In the United States, a law was passed in 2022 allowing therapies to be approved without the use of animal models, provided their safety and efficacy had been verified using alternative methodologies deemed scientifically valid, such as a computational model. The US Food and Drug Administration (FDA) has launched a progressive strategy to increase the use of these alternatives and guidance to encourage their development. As Xavier Morató, director of clinical trials at the Ace Alzheimer Center Foundation in Barcelona, tells SMC Spain, this “does not eliminate the use of animals, but allows them to be partially or totally replaced when such methodologies demonstrate sufficient scientific validity and human biological relevance”. In any case, “animal testing is key to human safety and for establishing dosages”, the expert adds. Montoliu points out that the FDA retains the authority to require animal testing and that “Europe is not currently considering legislation of this kind. Although it proposes to explore the use of these alternatives to help reduce the use of animals, as they can provide very useful and complementary information, it does not yet allow for the complete replacement of animal use in the development of a therapy”, he explains.
Of the types of animals used in experimentation in Europe, 55% are rodents, and of these, the vast majority are mice. Their widespread use is due to several reasons: they are small and easy to handle, inexpensive, grow and reproduce quickly, have a fast metabolism and age rapidly, which facilitates various types of research. Furthermore, they share approximately 85 to 90% of their genetic information with humans and, in general, their systems and ours function in a fairly similar way.
What are its general limitations?
“Although they are mammals with which we share a remarkable genetic similarity, it is important to bear in mind that ‘mice are a distinct species; they are not simplified humans’,” warns Montoliu. Other more similar species, such as dogs and cats, provide examples of situations in which we differ in ways that are not entirely predictable: “Chocolate can kill a dog and paracetamol is highly toxic to cats,” explains the researcher. The main difference between mice and humans is “that the former, due to the environment in which they usually live, have developed much more powerful systems for eliminating toxic substances”. This means that many compounds which may be harmless to them are harmful to us. Furthermore, as we shall discuss later, there are differences regarding the mouse models used for each disease, the extent to which they are capable of accurately reproducing it, and the greater or lesser degree of reliability they may offer (and which, in any case, must always be confirmed).
“The treatments being tested do not necessarily work in the same way in mice and humans, but if it is confirmed that they do work in mice, there is a certain probability that they will work in us,” the expert summarises.
What are the phases of clinical research into a treatment? What is the average duration and probability of success for each phase?
The first stage in the development of a medicine is basic research, during which a candidate molecule is identified and characterised, its mechanism of action is studied, and its potential efficacy and safety begin to be assessed. Broadly speaking, of the approximately 10,000 compounds that are studied, only around 250 progress to the next stage, the preclinical phase.
The preclinical phase involves a more thorough study of efficacy and safety in cell models and laboratory animals. Of the approximately 250 compounds that reach this stage, only between five and 10 progress to be tested in humans. Generally, if news emerges about a drug that has been successfully tested in mice, it is at these stages of research. Overall, on average, it is estimated that the basic and preclinical phases last around six years, although this timeframe can vary considerably.
The next step is to study it in clinical trials in humans. To do this, it has generally had to be successfully tested in two different animal species. In addition to mice, “it may be in dogs, as in the case of gene therapy. When it comes to vaccines, it is mandatory to test them in non-human primates,” explains Montoliu. The move to clinical trials requires approval from an ethics committee, but is also subject to variables that affect the timeline or even whether the trial ultimately goes ahead: the commercial interest in the drug or the disease, whether the compound is protected by patents, whether it is administered on its own or must be used in combination with others that may be protected, amongst other factors. “Not all strategies tested in animal models translate into clinical trials,” points out Morató.
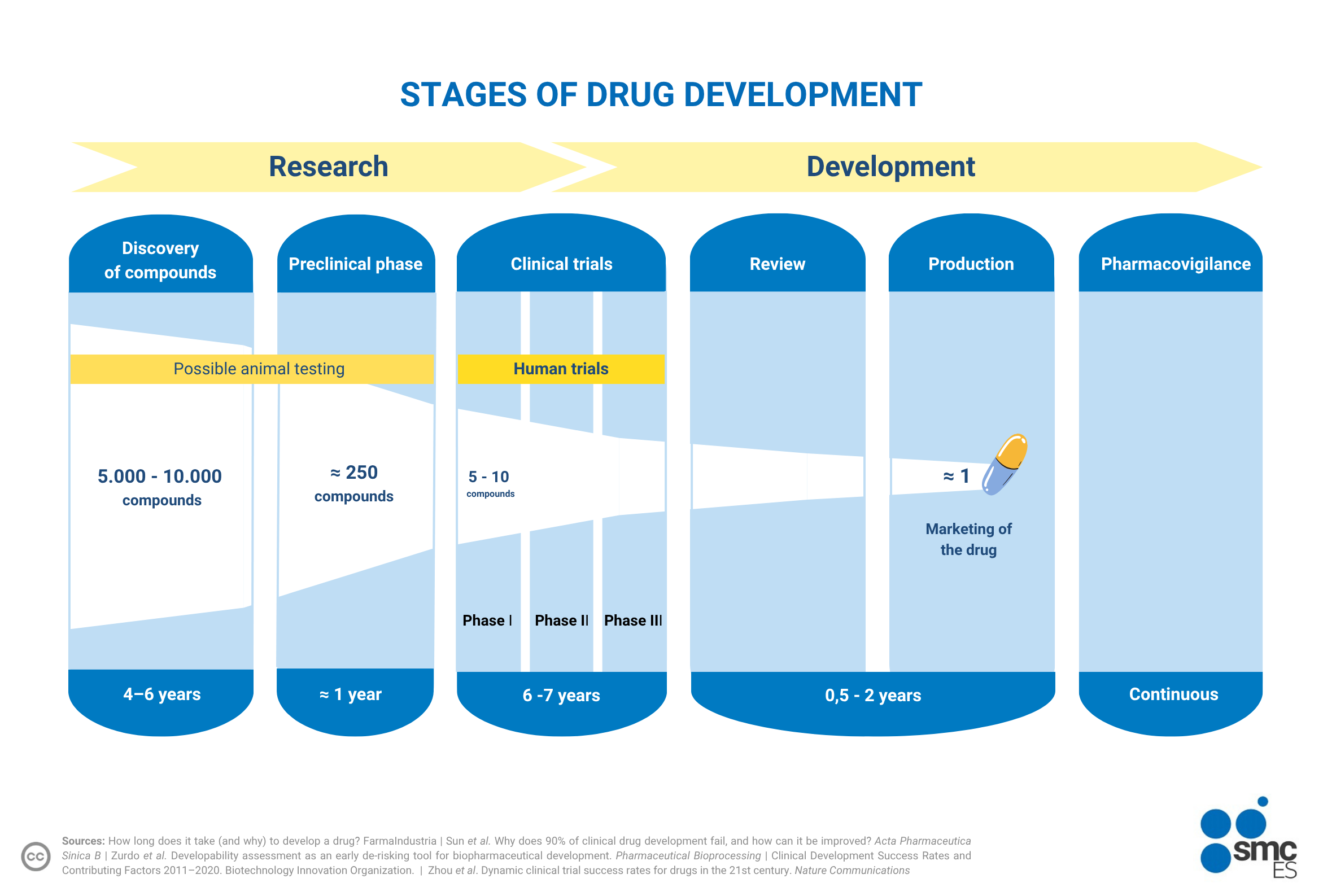
Clinical trials comprise at least three phases that must be successfully completed in order to obtain approval; this does not imply a cure, but rather that the trial has met the objectives set at the outset, which may vary depending on the drug or the disease. In general, it is estimated that only around 10% of compounds that reach this stage—after an average time of around six or seven years from the start of the process—will ultimately be approved, as stated in the AEMPS report How Medicines and Medical Devices are Regulated in Spain. Hence the numerical and general summary that is repeated in many articles: that 90% of clinical trials fail (mostly because they prove ineffective at a safe dose or, secondly, due to excessive side effects).
In short: if you read a news story about a therapy that has been successful in mice, you should know that this is a necessary first step so that, at some point, it may become useful in humans. But also that it is far from sufficient: that it will almost certainly need to be tested and trialled in another animal species; that a three-phase clinical trial strategy must be viable, designed and approved, with a success rate of around 10%; and that the average time from the emergence of evidence in animals until potential approval can be achieved appears to be, according to a recent study, around 10 years in total.
If it usually takes so long, a question that often comes up is: why were the COVID-19 vaccines approved in just two years?
The processes can vary depending on the type of compound and disease. In the case of vaccines, development usually takes between four and seven years, and the approval process takes around 10 years, although this is subject to variation. The timelines for COVID-19 vaccines were shortened to approximately 10 months and just under two years, respectively. One of the key factors, explains Montoliu, is that a great deal of groundwork had already been done. In the case of RNA vaccines, “research had been ongoing for 15 years and the framework was already in place; they were practically ready to go”. But, above all, because they were developed during the pandemic and thanks to the huge number of volunteers, “the clinical trials had a statistical power never seen before and any potential side effects could be identified much more quickly”.
Do all drugs entering clinical trials have the same chance of being approved? Does this vary depending on the disease?
In general, depending on the type of compound and the disease it targets, the initial probability of it eventually being approved varies on average. According to a report that assessed the clinical development of nearly 10,000 therapies from almost 1,800 companies between 2011 and 2020, the highest probabilities were for those related to haematology, metabolic diseases and infectious diseases, with success rates of approximately 24%, 15% and 13%, respectively. At the other end of the scale, some of the areas with the lowest success rates were neurological and cardiovascular diseases and cancer, all at around 5%. In general, those considered chronic and common, or of high prevalence, had a success rate of approximately 6%. The stage at which most therapies tended to fail was during the transition between Phase II and Phase III trials.
Various factors can also influence these figures. The most novel drugs tend to have a lower probability of success, and there can be significant variation within each disease area. For example, the probability of approval for pancreatic cancer was 1.1%, whilst for gastrointestinal cancers it was 15.2%.
Overall, the global success rate was 7.9%, slightly lower than the theoretical 10%. The average time taken to complete the entire process was 10.5 years.
When we say that a mouse is a ‘disease model’, what does that mean? Are all models similar? What are their limitations?
A mouse used as a disease model is one that has been selected or modified to replicate, to a certain extent, a human disease. Given that mice are not simplified versions of humans, there are always certain limitations when it comes to replicating all their characteristics. These are some of the main limitations in relation to some of the most prevalent and widely studied conditions, such as cancer, cardiovascular disease and Alzheimer’s disease.
-
Cancer models
There are various ways of studying tumours in mice. Some of these involve directly implanting tumour cells grown in the laboratory or introducing a mutation into the animal that causes the tumour. In general, these methods are limited, as they are far from resembling or replicating the variety of cancer found in humans. Other, more advanced methods involve implanting part of a patient’s tumour into the mouse, either under the skin or, preferably, in the same organ from which it originated, in order to better mimic its environment. However, this also has its limitations: only a part can be used, which does not represent the whole and may develop differently; and, above all, it is usually necessary to do this in mice without an immune system, so that their defences do not attack it and prevent its implantation.
“This is a problem,” Ignacio Melero, Professor of Immunology at the University of Navarra, researcher at CIMA and co-director of the Department of Immunology and Immunotherapy at the University of Navarra Clinic, acknowledges to SMC Spain, because it limits the similarity to humans in a very significant respect and, furthermore, “does not allow for the evaluation of immunotherapy treatments”. Although, on occasions, “mice can be humanised, this often poses a problem for large-scale research”.
Furthermore, and in general, mouse models are not perfect when it comes to reproducing the environment in which the tumour grows or its behaviour when it metastasises.
-
Models of cardiovascular disease
Atherosclerosis is the leading cause of cardiovascular disease, which is why countless studies have been carried out on mice to understand and reduce it. Although these have led to significant advances, they also have their limitations. For example, mice are highly resistant to it and rarely develop the condition; consequently, they generally need to be genetically modified and sometimes fed a very high-fat diet in order to study it. Furthermore, although the lesions are similar, they are not the same as those in humans. And, unlike what happens to us, most of their cholesterol is in the form of HDL, the so-called ‘good cholesterol’.
-
Models of Alzheimer's disease
Mice have many limitations when it comes to modelling Alzheimer’s disease. Generally, models are created by increasing the expression of a specific gene, but most cases in humans are more complex. The simultaneous accumulation of amyloid plaques and tau protein that characterises the disease does not usually occur accurately in mice, and as Morató explains, these “do not adequately reproduce the role of ageing, neuroinflammatory responses or vascular contributions”. Furthermore, “cognitive deficits in mice are assessed using simplified tests that do not capture the complexity of human decline. All of this may go a long way towards explaining why many findings do not translate well to the clinical setting,” he concludes.
Furthermore, and in general, a problem with research in mice is that, as related animals are bred together, there is very little genetic variability. This facilitates the standardisation, verification and reproducibility of results. However, “a few changes can already lead to significant differences, and in humans we will find much greater variability. We must be sceptical and cautious about the system in general”, summarises Montoliu.
Are all animal studies of the same quality? Does the fact that a study is conducted on mice make them all the same?
No, there is considerable variation in the quality and reliability of studies conducted on mice, which also raises concerns within the scientific community. One of the problems is that, for ethical reasons, researchers tend to use as few animals as possible, “and that can reduce the study’s statistical power. There is a delicate balance between reducing their use and the reality of research,” explains Montoliu. Furthermore, the quality of research can vary depending on its design, the statistical analyses employed, the tests carried out to avoid potential biases or confounding factors in the results, whether male and female animals were used—as sex can influence certain results—and so on. And, as we have seen, differences may also arise in the interpretation and reliability of a study depending on the disease and the knowledge of the compound under investigation or the mouse model used, however good it may be among those available.
In any case, when a study in mice is published, and regardless of its supposed quality, the initial reaction should always be one of caution. Any research must be tested in humans, and its translation is far from automatic.
How, then, should these studies be communicated and interpreted? Is it enough simply to state in the headline that they were conducted on mice?
“A headline that omits the fact that the research was carried out in mice may be more eye-catching, but it is essential to include this information and resist drawing hasty conclusions,” says Montoliu. Including the phrase “in mice” in the headline is necessary, but may not generally be sufficient. It is important to bear in mind that this fundamental caveat does not grant carte blanche, and that the reader’s own emotional response may alter how the text is interpreted. A delicate balance must be struck between the information provided and the implicit promises.
A headline that fails to mention that the research was carried out on mice may be more eye-catching, but this detail must be included
Lluís Montoliu
“It must always be emphasised that these studies are carried out in an animal model and that this only partially replicates how things work in humans,” stresses the researcher, who also points to the responsibility of scientists, who, when presenting their projects and seeking funding, must justify their impact and sometimes make “pie-in-the-sky claims”. Animal models “involve a great deal of uncertainty, but they are the tool we have and we must use them with caution”, he summarises.
As Folkman already knew, “history is full of cases where treatments that have been successful in animal models have not worked in humans,” recalls Melero, for whom “we must be very cautious, both in terms of information and in scientific publications themselves, which must be completely transparent”. The key, according to the expert, is “being able to communicate advances that are considered important in a simplified, but not simplistic, way, explaining the limitations, the need for clinical trials, whether these are expected to take place, and the estimated timeframe for their completion”. He concludes: “It is essential not to create false expectations among today’s patients”.




