Anti-amyloid drugs for Alzheimer's disease have not been shown to have clinically significant effects, according to a Cochrane review
A review of studies conducted by the Cochrane Collaboration analyzed data from 17 clinical trials involving more than 20,000 participants who had been treated with amyloid-targeting drugs—such as lecanemab or donanemab—at a relatively early stage of Alzheimer’s disease. Results at 18 months of treatment show that “the absolute effects on cognitive decline and the severity of dementia were nonexistent or negligible, falling well below the thresholds established for a clinically meaningful difference,” according to a press release. Furthermore, the review concludes that these drugs likely cause more brain inflammation and microbleeds than the placebo.
Jordi Pérez-Tur - Alzheimer med
Jordi Pérez-Tur
Research scientist at the Public Research Organisation (PRO) at the Institute of Biomedicine of Valencia of the Spanish National Research Council (CSIC) and principal investigator at CIBERNED
Abstract
This review evaluates the clinical benefits and risks associated with the use of anti-Aβ monoclonal antibodies (anti-Aβ mAbs) in individuals with mild cognitive impairment (MCI) or mild Alzheimer’s-type dementia, an early stage of the disease.
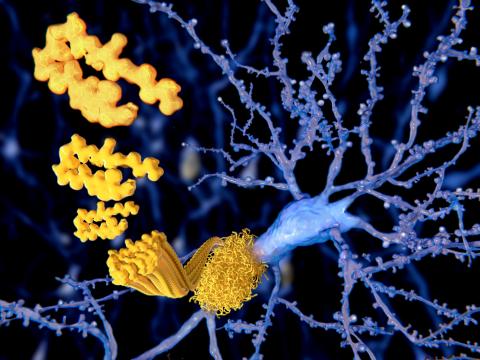
Alzheimer’s disease is an incurable cognitive disorder typically associated with aging that arises from neuronal death in various brain regions. Initially, it affects the hippocampus and associated regions, leading to memory problems; however, over time, the disease progresses and affects different areas of the brain. Neuronal death, which only produces clinical symptoms once a significant number of neurons in these areas have already been lost, is linked to the formation of extracellular Aβ deposits and intracellular tau protein deposits, in both cases accompanied by other molecules.
This is a disease for which only symptomatic treatment is available—a treatment that is very ineffective and, in some individuals, manages to delay the progression of the disease by a few weeks or months.
Recently, a new class of treatments based on monoclonal antibodies against Aβ has been approved. The idea behind this treatment is that the antibodies can “tag” Aβ deposits and thereby activate the cellular machinery responsible for removing that peptide from the brain.
This review has analyzed the effect of the various anti-Aβ mAbs currently on the market, as they all act similarly and focus their mechanism of action on the same process: binding to the Aβ peptide and its removal from the brain environment. It is worth noting that the approval processes for these treatments, particularly in the case of the first ones—aducanumab and donanemab—were not without some academic controversy, as several members of the FDA and EMA approval committees assessed that the clinical effect was very limited. Ultimately, following a review of the treatments’ efficacy criteria and their effects, the first two were approved, followed by the rest. In this regard, this review is timely as it addresses an issue of great clinical relevance.
Using a methodology common in meta-analysis studies, they conclude that, 18 months into treatment, they observe little or no difference in cognitive function between treated individuals and those treated with placebo. Using improvement on the ADAS-Cog SMD test as a criterion, they observe that treated individuals show a very slight improvement (of less than 1 point, when a change of at least 2–4 points is considered necessary). If the effect is analyzed at 24 months, the result is even more uncertain. This minimal or no effect is also observed with other measures of cognitive function. The authors conclude that these slight improvements on various tests were unlikely to translate into significant improvements in daily functioning or the ability to maintain a certain degree of independence.
On the other hand, these treatments also have side effects, such as amyloid-related imaging abnormalities (ARIA), which occur more frequently in treated individuals, while other adverse side effects did not occur more frequently than in individuals treated with a placebo.
Finally, carriers of the e4 allele in the APOE gene have a higher probability of developing ARIA. This allele is the primary known genetic risk factor for Alzheimer’s disease, and a relatively high number of people with the disease carry this allele. This review was unable to analyze the role of this gene in treatment effectiveness in sufficient detail because, despite this evidence, many studies did not perform genotyping of participants due to the family implications involved.
Quality of the study
The “Cochrane,” as it is commonly known, is an international nonprofit organization dedicated to producing high-quality evidence to support health decision-making. Its most renowned output is the Cochrane Systematic Reviews, regarded as the gold standard for summarizing health evidence. These reviews are conducted using a specific structure and focus on evaluating existing evidence and assessing the risk of bias in published studies. Their reviews are routinely used by international organizations (WHO, EMA, FDA) and various national committees. Furthermore, the reviews are periodically updated as new evidence emerges, reinforcing their clinical relevance.
This study follows the organization’s rigorous review process.
Implications, fit with existing evidence
The implications of this study are clear from a public health management perspective. The annual cost of these treatments is around €25,000. If there is no evidence that they have a significant clinical effect, does it make sense to continue using them? During the approval processes for these treatments, pressure from companies and patients played an important role in bringing them to market, but there were many experts who recommended against their approval. As evidence accumulates regarding their use, it is becoming quite clear that the benefits are extraordinarily limited. And we do not yet know if they are sustained over time. The only remaining question is what happens if patients are stratified based on the presence of certain genetic risk factors.
Limitations
The study itself has no greater limitations than those of the studies on which it is based. Thus, the authors note that the results cannot be generalized to the entire patient population, since the average age at onset is around 80 years, while the groups studied in the review have an age at onset ranging from 69.5 to 73.9 years. Furthermore, the follow-up period is relatively short. The authors also identify some limitations related to the studies analyzed, such as the fact that many of them are funded by the pharmaceutical industry that produces these treatments.
Regarding the study itself, the authors do not identify any limitations concerning the analysis performed.
General comments
This study represents an effort to demonstrate, based on the publications emerging regarding the efficacy of these treatments, to what extent this therapy is effective. It is to be hoped that in the coming months we will see an update to this review that includes follow-up over longer periods, with more diverse populations—not just predominantly of Caucasian origin—with greater detail on the genetic profile of the participants, and with ages closer to those of the general patient population.
Xavier Morató - Cochrane alzhéimer EN
Xavier Morató
Director of Clinical Trials at Ace Alzheimer Center Barcelona
This Cochrane paper, recopilates 17 RCT including different drugs, with demosntrated different capacity for amyloid removal. A strong, positive correlation exists between amyloid-beta plaque removal and clinical efficacy in early Alzheimer’s disease, with greater plaque reduction leading to slower cognitive and functional decline.
In anti-amyloid antibody treatments, reducing plaque to a negative Amyloid PET scan level is not strictly required to observe a clinical effect, but it is highly correlated with greater benefits. Studies show that treatments like lecanemab and donanemab show significant plaque removal and slowed cognitive decline (about 27–35%) even before reaching fully negative PET levels, though maximum benefit is seen when patients reach amyloid-negative status. It is also important the velocity of amyloid removal. Both Lecanemab (55 centiloids in 18m) and DOnanemab (88 cetiloids in 18m) are the best mAbs described in the market with otther mAbs such as Trintinemab (90 centiloids in 3m).
Brodtmann - Amiloide
Amy Brodtmann
Neurologist, professor and director of the Cognitive Health Initiative at the School of Translational Medicine, Monash University (Melbourne, Australia)
The authors concluded that the effects of these therapies on cognitive function and dementia severity were trivial to small, while increasing the risk of adverse events such as brain swelling and bleeding. The findings concord with the decisions of several international governmental agencies to deny approval based on efficacy, including the Australian PBAC, but differ from others, such as the USA.
Cochrane reviews represent the highest standard of evidence-based healthcare. They have included all major trials published to 7 August 2025. However, the inclusion of older trials known to be negative does skew the findings somewhat, as we know that these agents had less amyloid clearance than newer agents. It would have been interesting to have a pooled analysis of the 3 agents with positive trials, aducanumab, lecanemab, and donanemab.
In addition, their sobering conclusions that “Successful removal of amyloid from the brain does not seem to be associated with clinically meaningful effects … future research … should focus on other mechanisms of action” will be contentious. The Alzheimer’s disease field still contains a solid majority of adherents to the amyloid hypothesis, and these comments will spark intense debate. However, there will be many clinicians who welcome this objective guidance for evidence-based care.
Conflicts of interest: Scientific Advisory Committees Eisai (lecanemab), Lilly (donanemab), Roche (gantenerumab). Paid travel to Australian Dementia Research Forum June 2025. Honorary Medical Advisor Dementia Australia. AFL Brain Health Collective Committee Member.
Tara - Cochrane
Tara Spires-Jones
Director of the Centre for Discovery Brain Sciences at the University of Edinburgh, Group Leader in the UK Dementia Research Institute, and Past President of the British Neuroscience Association
This review by Nonino and colleagues examined data from randomized control trials of antibodies to amyloid beta, one of the proteins that clumps in the brains of people with Alzheimer’s disease. While reviewing clinical trial data is useful, the authors of this study combined analyses of 5 drugs that did not succeed in their trials and 2 drugs that did succeed in slowing disease progression and have been approved to treat early Alzheimer’s disease in several countries. The authors’ conclusion that anti-amyloid antibodies do not provide clinically meaningful benefits is weakened by including 5 drugs that did not pass their clinical trials and are not available. Emerging data on long-term use of the approved drugs and careful analyses by regulators including the European Medicines Agency and UK Medicines and Healthcare products Regulatory Agency (MHRA) support the use of two amyloid antibodies, lecanemab and donanemab, to slow decline in early Alzheimer’s disease. As the authors of this study point out and as was previously published in the original trials, these drugs are not perfect, they come with risks of serious side effects and only modestly slow progression. Due to the limited benefit and high costs accompanied by risks of brain bleeding and swelling, these drugs are not covered by the NHS. However, newer research into both more advanced amyloid targeting drugs and other targets shows promise for improved treatments on the horizon.
Conflicts of interest: "I have no conflicts with this study but have received payments for consulting, grant reviews, scientific talks, or collaborative research over the past 10 years from AbbVie, Sanofi, Merck, Scottish Brain Sciences, Jay Therapeutics, Cognition Therapeutics, Ono, Novo Nordisk, Eisai, and Boehringer Ingelheim, and direct a company Spires-Jones Neuroscience, Ltd to act as a consultant. I am also Charity trustee for the British Neuroscience Association and the Guarantors of Brain and serve as scientific advisor to several charities and non-profit institutions".
Nonino et al.
- Research article
- Peer reviewed
- Review